The preliminary sign from a tooth sprain is pain. Dental practitioners particularly try to find dull or achy pain as sign of a ligament sprain. You might also experience a sharp, localized pain in one tooth.
Modern Dentistry, in all of its innovation over the last 50 years, has fixed much of the issues that have occurred with the increase of tooth retention.
However, circumstances still occur that reasonable professionals can disagree on diagnosis and treatment. Such, differences might lead to postponed reliable treatment, unneeded procedures, or actions that are excessive.
Pro Tip: This Portable Water Flosser is up to 50% more effective than traditional floss and can save you hundreds on professional dental cleanings. Its 300ml tank and cordless design make it perfect for maintaining healthy gums. Check the current deal on Amazon.
All create a circumstance of frustration for the patient and the dentist leading to ill will and ineffective activity.
Think about a typical example: A patient provides the following issues; dull generalized ache, periodic gum “itchiness,” pain when penetrating localized gum pockets, soreness to chew, sensitivity to temperature level, occasional headache.
The pain is not severe adequate to wake the client out of his/her sleep, but there is enough discomfort for the patient to make a particular appointment to go over the issue. In addition, the client recently had a cavity completed the area of discomfort.
A prudent course of action to identify the concern is to take an x-ray, temperature tests, percuss, and bite tests to separate potential issues which might be causing the pain. It is likewise affordable to check the client’s bite with articulating paper to figure out possible high spots.
Yet, common strategies do not appear to deal with or identify the patient’s problem. There are no cavities, cracked teeth, sinus issues, or acute pains related to biting.
Dental Care: This Rotating Electric Toothbrush removes up to 400% more plaque than a manual brush. With a built-in pressure sensor and 8 replacement heads included (a 2-year supply), it’s a cost-effective way to maintain a professional clean at home. Available on Amazon.
There are medical signs of a molar rise with a lateral trip on the client’s working (chewing) side and likewise a balancing side contact on the very same tooth with the opposite lateral adventure.
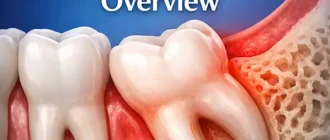
Besides, the tooth is somewhat mobile, and the gum tissues are tender and bleed upon penetrating. The x-ray does indicate a somewhat thickened periodontal ligament space and a somewhat thickened layer of the cortical plate surrounding it, but no bone loss appears.
At this moment, affordable practitioners would disagree on the next steps to take. Some might try to correct the problem by submitting the tooth down or replacing the filling, others may perform a root canal or crown, a few would even think to extract the tooth, and some might do nothing.
This paper proposes an alternative point of view to resolve such symptoms, enabling the dentist a possible diagnosis and possible treatments. Such, a diagnosis would be called “Sprained Tooth Syndrome.”
Sprained Tooth Syndrome Definition
For the function of this short article, Sprained Tooth Syndrome (STS) is specified as a condition where unusually strong bilateral opposing vector forces cause the ligaments connecting a tooth to the bone to end up being stretched and chronically irritated; hence creating patient discomfort similar to that which is explained above.
Just as ligaments can be extended and damaged in an ankle or other parts of the body, similar damage can occur with the ligaments linking a tooth to the bone resulting in STS.
What Causes of Sprained Tooth Syndrome?
Common causes that could result in STS are:
- Cold, sinus problems, or allergies
- Trauma from little objects (popcorn seed etc.)
- Filling or Crown overfilled.
- Filling underfilled.
- Drifting of teeth.
- Early essential tooth infection.
- Damage, wear, or improper repair to discluding working side teeth (canine rise or group function is preferable).
One typical reason for STS is tooth movement due to sinus problems or colds. Extreme swallowing as a direct outcome of sinus drain may result in irregular outside lateral pressure from the tongue to the teeth producing temporary orthodontic pressure and movement outside.
This temporary external shift of the tooth might place the lingual cusp in harm’s way of damaging lateral tooth to tooth forces. As such, it is essential to determine why the teeth are moving, causing horizontal friction to take place. In this case such as a cold or sinus condition, waiting for the client’s health to improve may be the best course of action.
After the cold has fixed there will be less tongue pressure and the cheek pressure will move the tooth back into a harmonious position.
Another reason for STS can be unintentional injury or trauma from little things such as a popcorn seed or a bone in a piece of meat.
This injury can cause momentary gum ligament damage and swelling which can trigger the tooth to supra-erupt into a damaging position which can then forever extend the inflammation.
Dentistry itself can promote these harmful conditions to occur in the mouth. If a crown is made with a best centric contact but cusps that hinder lateral excursive movements then STS can establish.
Similarly, if the centric contact of a filling or crown is left too low, with time (a few days to a few weeks) the tooth can supra-erupt and move one or more cusps into an occlusal interference which would result in STS caused inflammation.
Wandering teeth are always at risk of moving several cusps into this destructive lateral excursive pathway.
Sometimes a tooth infection can trigger supraeruption of that tooth, putting the cusps in damages way. The ensuing symptoms will belong of the Sprained Tooth Syndrome but secondarily to the tooth infection.
Once again highlighting the need to discover why a tooth has moved into this lousy position. In all cases of STS it is essential to follow up (2 wks, 4 wks, 3 mos., and 6 mos.) to ensure symptoms are dealt with and infection was not the root cause of the STS.
Lastly, a less apparent however similarly crucial reason for STS is the damage, wear or improper repair of the discluding (working side) teeth. It is this working side protection (canine rise is best) that keeps the stabilizing side cusps out of a problem.
Simply put, posterior teeth are designed to take in massive forces in the instructions of the long axis of the tooth. Most posterior teeth are not created to soak up damaging lateral forces which can lead to STS. Identifying how these destructive forces have come about is essential in figuring out treatment.
Diagnosis
Identifying STS is not as necessary as it might appear. In some cases, symptoms may lead you to believe the issue is STS when in reality it is an early essential tooth infection.
A vital tooth infection is specified as an early infection of a tooth which has a nerve that is partially infected and partially crucial; hence releasing the very same symptoms and discomfort as STS.
A few practical tests should allow dental professionals the comfort that they have adequately diagnosed STS:
- Place a cotton roll or “Tooth Sleuth” over the presumed teeth and have the patient bite. Ask the patient where they think the problem is located. Also, ask if the bite pain is sharp or dull and throbbing. Dull and achy is a sign of STS. Often with this test, the patient is not sure if the pain is originating from the top or bottom.
- Use the perio probe on the gum tissue to discover the tender area or irregular gum pocket and observe the client for discomfort which might show inflammation. The gum tissue might be tender circumferentially, or sometimes it may be localized on one side of the tooth impacted.
- Percuss teeth with mirror deal with and observe the client for pain action which might show gum inflammation.
- Pulp test and cold test teeth. (a sprained tooth, unless it has been root canaled, might be sensitive to cold and ought to respond to a pulp test-possibly with an elevated reading pending any associated pulpal inflammation secondary to gum inflammation.)
- Place articulating paper over the affected teeth and have the client grind commonly right and left. Observe the markings. Any balancing side contact accompanied by a similar strength working side contact on the very same tooth spotted by this approach can lead you to think this syndrome.
How to explain STS to patients:
Individuals do not chew their food in a straight up and down movement. Instead, they chew on a hinge using a lateral envelope of movement.
A person’s cuspid/canine teeth must help to protect their molar cusps from banging versus one another throughout this motion.
Cuspids are long rooted, heavily strengthened in bone laterally, have actually slanted slope biting surface areas, and are positioned forwardly in the mouth. These features make the cuspid teeth perfect as the “kickstand” for the mouth.
All of these protective functions except the forward positioning are self-explanatory.
For instance, the mouth is much like a nutcracker. The further back you go in the mouth the more pressure is put in.
That is why it is so essential for the cuspids (which are located anteriorly) to bear the brunt of the chewing strokes to take the pressure off of the molars. If the cuspids fail to protect, then the molars will bump and grind and begin to wiggle.
When a post is wiggled back and forth in the ground, ultimately the post chills out, and spaces around the post can form.
The dental professional needs to restore protection for the molars by either developing the cuspids, adjusting the high spots from the cusps on the affected molars, or a few other approaches such as fabricating a nightguard/bruxing device or orthodontic repositioning.
The affected tooth is like a sprained ankle, and it will take a week or so to heal. When the patient goes back to chewing on the impacted tooth, they ought to start with soft foods first.
Also, headaches have known to have been triggered by muscle tension. STS may likewise be linked to a boost in grinding, muscle tension, and headaches. In some cases solving these bite, issues have resulted in less or no headaches.
Also, notify the patient that gum chewing and single side chewing will likewise worsen this syndrome.
STS Treatment
Dealing with STS is rather easy; the dental practitioner must eliminate the 2nd vector force on the tooth, leaving the centric contact! Strong bilateral opposing vector forces cause STS, so removing among the opposing forces is essential.
However, the elimination of the second vector force can be a complicated procedure.
The most typical technique is to mark the afflicted tooth/teeth in lateral excursive movements with articulating paper.
Figure out the level and origin of the issue. Then develop a treatment strategy that will correct the issue.
However, complications may emerge such as in a crossbite occlusal plan. As a basic guideline if more than 1-2 teeth are included, or if by adjusting the bite you will be producing new issues then you choose not to change the 2nd vector contact.
There is a body of evidence that contralateral balancing side contacts may be vital for condylar joint health. In such cases eliminating this contact might do hurt to the TMJ.
Structure up to the safeguarded occlusion on the opposite side of the mouth, producing a night grinding home appliance to decrease nocturnal damage or orthodontically correcting the bite might be much safer alternative treatments specifically if the patient does not present with any TMJ symptoms.
Opposing vector forces can appear in a buccal/lingual, mesial/distal, or any opposing vector instructions in between.
The treatment is still the same- securely remove the second vector force leaving the tooth in a stable position so that you do not need to keep adjusting the tooth/teeth every 6 months.
Successful treatment will be indicated by an instant sensation by the patient that the bite feels various and much better. They might say things like “The bite doesn’t feel so tight” or “My teeth move across each other far better.”
Between a few days and a week, the tooth will feel back to normal with a total resolution of the subjective symptoms. Headaches and grinding may be entirely gone.
This conservative treatment method is only for patients with mild to moderate pain that is typically manageable with ibuprofen.
Instruct the patient to call the office if symptoms are not fixed within four to 5 days since it could be a sign that there is an early essential tooth infection which might lead to more significant problems if neglected.
If the symptoms do not deal with or if they worsen then instruct the patient to contact your workplace right away and treat this tooth problem like an infection and prescribe your antibiotic of option followed by the suitable treatment.
When do you deal with?
When the reward exceeds the threat.
Common risks are:
1). Getting rid of healthy enamel unnecessarily, breaking through to dentin or pulp.
2) Changing the client’s bite to one that is less steady or would somehow intensify their condition. (The more symptoms that the patient has pre-treatment indicates that there is less danger that you will aggravate their condition.)
Decreasing Risk:
Limit the adjustment at 1-2 teeth. If it is moreover (or the occlusal scheme is complicated like for example a crossbite), then you require to think about ortho/jaw surgery, developing cuspids, restoring all posterior teeth impacted, or make a lifetime night guard. Jaw surgery and complete mouth restoration are the most invasive and ought to be thought about as the last hope.
If there are signs of opposing vector forces but no symptoms, then there is no benefit. In these cases, you enjoy it and encourage the patient what symptoms might emerge in the future.
If a client makes a devoted visit to address this problem, then there is a benefit to treating this case, and an effort is made to remove the 2nd vector force on the affected tooth. Most of the time the tooth and bite will feel 100% much better right away after changing.
Reward-you repair their pain, you make their bite feel much better, you validate their symptoms, you identify what others may have missed, you possibly assist cure their headaches, and perhaps prevent future gum problems (which is a debate for another paper) — all using a conservative, cost reliable method that expresses an authentic concern to solve their issue. The client can’t assist but to be grateful if it achieves success and it becomes a significant practice home builder.
Liability of not treating — The patient’s symptoms, possible periodontal damage, and psychological disappointment continue. You might lose the client looking for yet another viewpoint.
Follow-up is important for 4 factors:
1) To make sure the issue is solved to the patient’s satisfaction.
2) It offers you another chance to gather information referring to the problem which will help you localize and treat it.
3) To ensure that an early significant tooth infection can be eliminated. If symptoms are permanently pursued 2-3 months, then you can presume that there is no infection but you still x-ray the tooth at the 6-month recall.
4) It reveals the patient that you care and are listening to their grievances.
Q&A
What does a sprained tooth feel like?
Severe pain is a catalyst for self-diagnosis, which means that it is almost impossible for a patient not to notice a dislocation. The dentist’s office conducts a visual examination, which is often sufficient to determine the clinical picture and prescribe treatment. In some cases, X-ray examination is required – panoramic orthopantomogram or dental scan. Without timely diagnosis and treatment of the dislocation there is a high risk of complications, in particular, granuloma, root cysts can form inside the pulp.
What should I do if my baby’s milk tooth is sprained?
When a baby tooth is sprained, you should immediately visit your dentist, who will diagnose the problem and determine the next course of treatment. In the case of a partial dislocation, the tooth is usually fixed with a metal splint or a plastic mouth guard.
Do periodontal ligaments heal?
Yes, with the appropriate treatment. At the same time, you have to understand that this is a long process, because the strained tooth will in any case be under stress from the chewing process.
How long can a sprained tooth last?
The STS treatment process can take a week or longer. In order to speed up the process, dentists recommend the use of overnight mouth guards, a special liquid diet, etc. As we answered earlier, constant stress on the big tooth makes things worse and can even cause pain in the neighboring teeth as well.
Conclusion
There are lots of patients who are struggling with this syndrome. It is inadequately comprehended because several factors contribute to its start and intensity:
1) Bilateral opposing vector forces from occlusion-of which premature contacts and strange adventures can be very complicated and hard to find.
2) Biting force magnitude of which position in the mouth, steepness of cusps and muscular advancement are directly related and similarly challenging to identify or measure.
3) A frequency of the offending force-of which gum chewing, frequent consuming, single-sided chewing, or frequency of grinding is necessary danger aspects.
Several factors reduce the impact of this syndrome medically:
1) Pain tolerance.
2) Blood flow to the area for repair work of the inflamed tissue.
Regardless of how unknown this syndrome appears, after reading this article, it should be clear that unidirectional forces are endured better by teeth than bidirectional opposing vector forces. Furthermore, a dentist ought to have the ability to determine and deal with patients who present with symptoms and signs of the Sprained Tooth Syndrome.