TMJ-related headaches differ from the usual headaches in their localization and intensity.
TMJ stands for temporomandibular joint, which gives insight into why we may experience headaches of this kind.
An important part of dental treatment is the control, diagnosis and treatment of pain, as well as the management of its underlying causes. However, most dental patients with symptoms of pain of unexplained etiology often succumb to inappropriate diagnosis and, as a result, misdiagnosis and ineffective treatment. As a result, the patient not only continues to suffer from chronic pain, but also becomes frustrated with the dental treatment provided.
TMJ Headaches in the Maxillofacial Area
TMJ headaches are often felt closer to the facial area. By definition, maxillofacial pain (orofacial pain) is associated with localization to the soft and hard tissues of the head, face and neck. During painful stimulation of these areas through the structure of the trigeminal nerve impulses reach the corresponding centers of the brain. In the brain, such signals are interpreted “as unpleasant sensitive or emotional sensations resulting from actual or potential tissue damage. The density of tissue in the affected area greatly complicates the procedure of making a correct diagnosis. Quite often, patients describe the location of a toothache away from the actual lesion. The phenomenon of reflected pain is justified by the intertwining of multiple sensory nerve endings, which are directed to the trigeminal nucleus from the skin and deep tissues of the head and neck.
Toothache is one of the most common forms of pain in the maxillofacial region. Pain from temporomandibular joint (TMJ) dysfunction and headaches are the next most frequently reported. Often a patient may have pain of several etiologies at once. The difficulty in diagnosing the underlying pain is also due to the possible concomitant development of fibromyalgia, chronic fatigue syndrome, or other pathological conditions. In such cases, the best way to make a diagnosis is to use the “peeling the onion” principle – to verify changes in symptoms one by one.
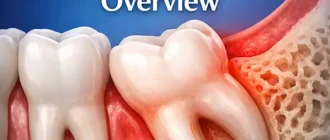
Temporomandibular joint understanding
To understand TMJ headaches, consider the function of the joint itself. The temporomandibular joint (TMJ) is a complex joint that provides both rotational and gliding movements of the lower jaw. Structurally, it consists of the mandibular condyle, which corresponds in shape to the articular fossa of the temporal bone. The articular disc of dense fibrous cartilage excludes direct contact of the bone surfaces. There are no blood vessels and nerve endings in the anterior part of the disc, while its posterior part, on the contrary, is characterized by an abundance of these structures. The joint is lubricated by a special synovial fluid that is in its composition. Movements of the TMJ are provided by the masticatory muscles. The other main type of muscle that does not take part in the development of TMJ movements, but is responsible for the demonstration of emotions, are the mimic muscles. The complex of masticatory muscles includes the masticatory muscles proper, temporalis, medial wing muscles, and lateral wing muscles.
Temporomandibular joint disorders
TMJ headaches do not appear by themselves, they have their triggers – these are diseases associated with the temporomandibular joint. Temporomandibular joint disorders are a group of musculoskeletal and neuromuscular disorders that predominantly affect the function of the joint itself, the masticatory muscles, or the articular disc. The possibility of TMJ disorders should be considered when making differential diagnoses of facial pain, since TMJ dysfunctions are the most common cause of pain in the jaw region of neodontogenic etiology.
To make a correct diagnosis, the patient’s history should be carefully studied, taking into account the parameters of pain onset and duration, as well as the factors associated with pain relief or worsening. In addition to persistent pain in the projection of the jaw, patients often complain of ear pain, headache, and diffuse facial pain. In addition, they may complain of an irradiated pain or stiffness in the face, jaw, or neck area associated with restricted jaw movement, the presence of painful clicking or cracking during closing or opening of the mouth.
Patients may also indicate changes in the relationship of the teeth to each other. The above symptoms may be particularly pronounced early in the morning, or worsen throughout the day. The threshold, localization, pain sensitivity, and description of pain sensations differ from patient to patient, and if we consider the complex mechanism of pain impulse formation, one thing is clear – diagnosis is a very important step to objectify painful changes.
The anamnesis remains one of the key aspects of comprehensive diagnosis, helping to detail aspects related to the development of pain. In addition, during the collection of the anamnesis when talking to the patient, the physician can visually assess the nature of lip and jaw movements, facial expressions and posture, as well as their emotional status.
Historically, occlusal disorders have been regarded as the primary cause of TMJ dysfunction. However, according to recent studies, these constitute only a small portion of the cases associated with painful joint dysfunction.
There are many classifications of TMJ dysfunction. In other words, pain in TMJ dysfunction can be arthrogenic and myogenic. Arthrogenic (joint and disc) TMJ dysfunction is usually caused by disc displacement or develops secondary to degenerative disc changes, ankylosis, dislocation, infectious lesion or neoplasia.
Myogenic dysfunctions occur due to muscle overactivity or as a result of bruxism, hypermobility or external stimuli. Myogenic joint dysfunctions can cause ischemia of the skeletal muscles of the face. Irreversible myocyte damage develops already after 3 hours of ischemic state and in parallel with microvascular progressive disorders. All this only adds to the pathological cycle of the facial pain development mechanism.
Patients with myogenic TMJ dysfunction are characterized by the development of more complex pathological disorders and more pronounced pain sensations compared to patients with arthrogenic dysfunction. That is why the main principle of joint dysfunction treatment is focused on the treatment and management of masticatory muscle hyperactivity.
Myollicular pain syndrome
One of the most common causes of TMJ-related headaches is myolitic pain syndrome. According to the National Institute for Dental Research, the most common form of TMJ dysfunction is myollicular pain syndrome (MPS). In this chronic inflammatory condition, not only the muscles but also the fascia are affected. The primary causes of this disorder are repetitive motion, lesions of muscle fibers, and excessive tension of ligaments and tendons.
Patients themselves often complain of a depressed state and fatigue, and even during the clinical examination the doctor may note some changes in their behavior. The differential sign of MBS is the presence of the so-called trigger points, the activation of which provokes the development and irradiation of pain in different parts of the head and neck.
Trigger points are formed in the projection of excessive muscle contraction and dysfunction of one of the components of the biomechanical complex of the head and neck. This type of muscle spasm differs from physiological tension of the whole muscle: due to local excessive contraction, blood flow directly to the area of contraction stops, which consequently leads to the development of ischemia.
Accumulation of metabolic products and toxins sensitizes the trigger point, essentially “forcing” it to send pain signals to the brain, which provokes even more contraction. Thus, the mechanism of trigger point formation involves a vicious circle of metabolic crisis. Clinically, trigger points can be identified by analyzing existing signs of the lesion, reproducing symptoms, and performing palpation. Deep palpation almost always identifies the main trigger points. Often, the patient may experience muscle twitching when pressure is applied to the trigger point.
Chewing muscle vs. TMJ Headache
If there is a problem with the masseter muscle, you may observe pain radiating to the temporal area. The chewing muscle is the main muscle of the whole masculatory muscle complex. The lower jaw is the only moving part of the skull, whose movements are ensured just by the chewing muscle. It is located in the parotid region on the posterior edge of the jaw, can be easily visualized and palpated by clenching the jaw.
The average person can bite with a force of 150 pounds, but a bite force of more than 250 pounds is also considered normal. This strength of the masseter muscle is achieved due to specific biomechanical conditions: its leverage arm is much shorter than in other muscles.
Taking into account the high activity of the masticatory muscle, its tensions are visualized even when the emotional state of a person changes. When the tension in the muscle continues for too long a period of time, it provokes the formation of the very trigger points associated with myolitic pain. When trigger points are located in the projection of the masseter muscle, the patient may experience pain in the eyes, on the surface of the face, in the structure of the jaw and teeth.
According to Simons and colleagues, the masticatory muscle trigger mechanism may even be responsible for the development of pain and itching in the ear structure, as well as the development of tinnitus – an unreasonable ringing in the ears.
It should be remembered that facial nerve is motor and is responsible for innervation of facial mimic muscles. Consequently, when treating trigger points in the deep layers of the masseter muscle you need to take into account the specific anatomy of the facial nerve in the projection of the zygomatic arch.
Headache and Temporal Muscle
Headache referred to TMJ can be caused by pathology of the temporalis muscle. The temporalis muscle is a large, thin, fan-shaped muscle located on the side of the skull above and in front of the ear.
Although the masseter muscle is considered the most powerful, the temporalis muscle also plays an important role in the chewing process. It starts from the temporal bone of the skull and runs completely under the zygomatic arch (zygomatic bone), attaching to the mandible, thus assisting the chewing muscle in closing the jaw and retracting it. By placing your fingers just above your ear, squeezing and unclenching your jaw, you can feel the biomechanics of the temporalis muscle. Trigger points in the area of the temporalis muscle are associated with the possibility of developing pain in the projection of the upper teeth, head, cheeks, eyes and ears. Doctors often resort to endodontic treatment if the nature of the pain is misdiagnosed, although it may be of a completely non-dontogenic nature.
Treatment of TMJ headache by botulinum neurotoxin type A
Chronic TMJ headaches sometimes have to be treated with BoNT-A injections. Given the basic principle of “do no harm”, the treatment of myolitic pain should be carried out by implementing noninvasive and reversible methods of intervention. Various palliative approaches and their combinations may be used to relieve TMJ dysfunction, which include but are not limited to splint therapy, massage, physical therapy, biocontrol, acupuncture, chiropractic, ethyl chloride sprays and stretches, use of antidepressants, narcotic and nonsteroidal anti-inflammatory drugs.
In addition, botulinum neurotoxin type A (BoNT-A), which is widely used in cosmetology (Botox, Dysport, Xeomin) and which has been pre-approved by the FDA for the treatment of painful conditions potentially associated with TMJ disorders (neck muscle dystonia, migraine, etc.) can be used. BoNT-A is an injectable pharmaceutical agent that is derived from the bacterium Slostridium botulinum. In low doses, this purified protein can be used to achieve selective relaxation of skeletal muscles because it prevents the release of acetylcholine in the neuromuscular junction. Consequently, this prevents the muscle from contracting with the same intensity as the amount of neurotransmitter available decreases.
Constant, sometimes dysfunctional contraction of the masticatory muscles may be the main reason for the formation of trigger points in TMJ-associated disorders associated with myolitic pain syndrome. Treatment of TMJ dysfunctions with BoNT-A lasts for a month, allowing the effect to be achieved for 3-4 months.
The physiological functions of chewing, speech, swallowing remain intact, but the intensity of pain is markedly reduced.
Unlike systemic drugs, botulinum toxin acts only locally, allowing to stop both active and latent trigger points. Immediately after the injection, the patient can report immediate pain relief as a “dry injection” effect develops. Although the cause of the pain dysfunction cannot be cured with this approach, the effect of BoNT-A injections becomes more lasting over time.
On the other hand, if other treatments are resistant, this approach can provide a successful alternative for relieving existing pain.
Dentists who are considering using BoNT-A in their practice as an approach to relieving pain associated with TMJ dysfunction should receive specialized training. During the latter, the doctor will be able to become familiar with the features of anatomy, physiology, pharmacological characteristics, as well as adverse reactions and potential complications associated with the use of botulinum toxin.
The average price of a vial with 100 units of active ingredient for a physician is about $600. Before using BoNT-A, you should also consider the specifics of local laws regarding the performance of such manipulations.
Bruxism and Dental Sleep Medicine
Induced headaches due to incorrect jaw function during sleep are also not uncommon. Dental parafunction is a habit that causes certain organs of the mouth or jaw apparatus to malfunction. It has nothing to do with water or food intake or with speech function. The most common parafunctions remain bruxism, clenching, and pathological erasure. All are potentially related to TMJ dysfunction.
The physiological pressure applied to a tooth ranges from 20-80 psi (0.14 to 0.55 MPa), while in bruxism it can be as high as 300-3000 psi (2.07-20.7 MPa).
It is logical that under such conditions, the load on the masticatory muscles also increases significantly, and their overload, in turn, leads to the development of myolitic pain syndrome.
Hypertrophy of the masseter muscle
Sometimes head (facial) pain caused by hypertrophy of the masseter muscle can even cause facial distortion. When examining patients with facial pain syndrome associated with TMJ dysfunction, the dentist often identifies the presence of trigger points in the projection of the masseter muscle. In addition, such patients may have such severe hypertrophy of this muscle that provokes distortion of facial appearance.
This type of hypertrophy can be treated with the same BoNT-A injection protocol used in cases of TMJ dysfunction. Botulinum toxin injections reduce the intensity of muscle contractions, and allow the muscle to relax, eliminating the possibility of teeth clenching with excessive force. However, keep in mind that the goal of this treatment is not only to relieve pain, but also to normalize the visual shape of the face, the distortion of which was caused by hypertrophy.
Obstructive sleep apnea
Obstructive sleep apnea (OSA) develops when repeated episodes of complete or partial upper airway blockage occur during sleep. During an OSA episode, the diaphragm and chest muscles begin to work harder to open the blocked airways and allow air to enter the lungs. TMJ dysfunction and signs of nocturnal bruxism are often noted in patients with OSA. The American Academy of Dental Sleep Medicine classifies sleep bruxism as a movement disorder. It is reasonable to use a home monitoring device to record bruxism and OSA data. Important indicators are oxygenation level, heart rate, airway patency, presence of snoring, specificity of chest movements, and body position during sleep. Once a patient with bruxism has had an Apnea-Hypopnea Index score that could potentially indicate the presence of OSA, the dentist should contact the patient’s physician for a more detailed diagnosis. If OSA is mild to moderate in severity, a customized intraoral device can be fabricated for the patient to prevent the tongue from dropping and the lower jaw from dislocating, thereby keeping the upper airway clear.
Headaches
The link between sleep bruxism, TMJ dysfunction and headaches is well established. Headaches provoke the development of significant discomfort, disruption of normal daytime activities, and possible further chronicity of pain. About 30% of headache patients suffer from associated functional abnormalities and yet do not seek medical attention. Patients may describe signs of headache during history taking during a dental exam.
Tension headaches and migraine
Tension headache is the most common form of primary headache, occurring in most of the population at least once in a lifetime. The pain that develops from trigger points in the projection of the masseter muscle can be both episodic and chronic, and clinically it is quite difficult to differentiate them from migraine pain. Therefore, it is necessary to remember that Tension headache, as well as TMJ dysfunction, can be characterized by the presence of pain sensations, which are a variant of migraine, although they themselves consist of a migraine-like component. Sometimes there is a superposition of symptoms of several pathologies, which can be interpreted both as diagnostic criteria of TMJ dysfunction and as diagnostic criteria of the International Headache Society. The relationship between TMJ dysfunction and headache has been described in detail in the literature. Patients with an established diagnosis of Tension headache or migraine, which may be triggered by temporalis muscle myalgia, may also be characterized by the presence of symptoms characteristic of TMJ dysfunction.
On the other hand, patients who have been treated for TMJ dysfunctions also show a decrease in headache intensity levels. Recent data suggest that there is an increased prevalence of TMJ dysfunctions among patients with signs of vascular pain and migraines, as the latter can be interpreted as constituting a complex of pain sensations of specific localization. Also the potential role of facial nerve and facial muscle disorders should not be forgotten, which can also provoke the development of pain.
On October 15, 2010, the FDA approved the use of BoNT-A injections to prevent headaches in adults with chronic migraine. The treatment protocol involves selective relaxation of hyperfunctional masticatory or facial muscles. The treatment approach involves using the lowest effective dose necessary to alleviate pain; the dosage of the drug, however, depends on each individual patient’s individual response to the therapy being given. Again, dentists who are considering the use of BoNT-A injections are urged to take the appropriate practical training and to follow the principles of the available legislation. That said, the mechanism by which BoNT-A allows migraine pain relief is not entirely clear. It is believed that the botulinum toxin, by switching off the muscle tension, reduces the strain exerted on them, and thus relieves the pain associated with bruxism or clenching. However, the release of neuropeptides, especially the calcitonin gene-related peptide (CGRP), is considered an integral component of the pathophysiological mechanism of migraine. BoNT-A has been found not only to affect the autonomic nervous system, but also to directly reduce the amount of CGRP released by trigeminal neurons. On this basis, it can be assumed that BoNT-A also relieves headache through a direct effect on the central nervous system.
Cervicogenic headaches
Neck pain and neck muscle soreness are common symptoms of primary headaches. The diagnosis of cervicogenic headaches refers to cases in which the headache develops because of bony structures or soft tissue localized in the neck region. The pathophysiology of this condition is most likely related to abnormalities in one or more muscular, neurogenic, bony, articular, or vascular structures of the neck. Such lesions are often the result of head or neck trauma, but may also develop in the absence of a history of trauma.
Clinical signs of cervicogenic headaches may mimic symptoms of primary headache, Tension headaches, and migraine. The diagnosis of cervicogenic headaches can be made only after a thorough history and physical examination. Diagnostic criteria include one or more of the following symptoms: moderate to severe pain in the occipital, frontal, temporal, orbital region of the head, neck, and back; intermittent or chronic pain, usually deep and not pulsatile; headache triggered by neck movements; or limitations of neck movement.
Patients with cervicogenic headaches are usually characterized by a slight forward tilt of the head. Muscle trigger points are localized in the projection of the suboccipital, cervical and shoulder muscles, and with physical or manual stimulation they may provoke the development of headaches in the head area. Studies show that 44.1% of patients with cervicogenic headaches have myolitic pain syndrome associated with TMJ dysfunction. Moreover, when TMJ dysfunctions are treated, patients with cervicogenic headaches have a more effective pain management outcome, allowing patients to increase their range of motion of the neck as a whole. As with other pain symptoms associated with myolitic pain syndrome, they also respond well to BoNT-A injections.
Conclusions
TMJ dysfunctions are characterized by a set of clinical manifestations that are often painful and lead to limitations in physical activity. However, they are self-limiting and usually amenable to conservative treatment such as BoNT-A injections.
The main principles of treatment focus on reducing pain and restoring range of muscle movement, which helps to reduce existing physical limitations and relieves pain of an associated etiology. Treatment of TMJD dysfunctions also allows preventing tooth lesions and chipped restorations, pathological tooth mobility and periodontal tissue pathologies that may be associated with or caused by bruxism.
During the treatment of dysfunctions, some patients manage to get rid of nocturnal bruxism and relieve chronic pain in the neck and shoulder area in parallel. If signs of nocturnal bruxism are suspected, the patient should undergo a home monitoring procedure for potentially present obstructive sleep apnea.
Despite the generalized nature of head and neck pain, patients with chronic orofacial pain often primarily go to a dentist for care. Consequently, the dentist must be theoretically and practically prepared to treat TMJ dysfunctions and manage the pain associated with them in the course of his or her daily dental practice.