What does “loose teeth” mean in pediatric dentistry? Loose teeth in children can be a normal part of growing up—as primary teeth fall out to make way for permanent ones—or a sign of trauma, infection, or gum disease. In a nutshell, it’s either a no-brainer milestone or a red flag. According to the American Academy of Pediatric Dentistry, about 85% of kids naturally shed all 20 baby teeth by age 12 (Source: AAPD, 2024).
Most Common Causes of Loose Teeth in Children
| Cause | Percentage (%) |
|---|---|
| Natural Tooth Shedding | 55% |
| Oral Trauma | 18% |
| Poor Oral Hygiene | 10% |
| Gum Disease | 6% |
| Orthodontic Treatment | 5% |
| Nutritional Deficiency | 4% |
This chart shows the most common causes of loose teeth in children. Natural tooth shedding is the leading cause, followed by trauma and poor hygiene. Less frequent factors include gum disease, orthodontic treatment, and nutritional issues.
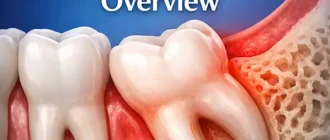
Why Do Children’s Teeth Become Loose?
Q: Are loose teeth always due to natural exfoliation?
Pro Tip: This Portable Water Flosser is up to 50% more effective than traditional floss and can save you hundreds on professional dental cleanings. Its 300ml tank and cordless design make it perfect for maintaining healthy gums. Check the current deal on Amazon.
A: Not always. While losing baby teeth is a hallmark of growing up, specific factors can trigger premature or excessive mobility. Key causes include:
- Natural Exfoliation:
- Timeline: Typically begins around age 6 and completes by age 12, with incisors shedding first and molars last.
- Mechanism: Root resorption occurs as the permanent tooth crown pushes upward, loosening the primary tooth.
- Trauma & Mechanical Forces:
- Acute Injuries: Falls, sports impacts, or playground accidents can displace or fracture teeth, causing immediate mobility. Such events account for roughly 10% of pediatric dental emergencies (Source: ADA, 2023).
- Chronic Stress: Habits like thumb-sucking, tongue-thrusting, or using teeth to bite hard objects may gradually loosen teeth over months.
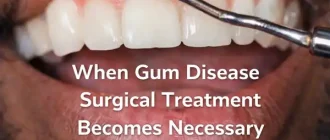
- Infection & Gum Disease:
- Gingivitis: Plaque buildup around the gum line leads to inflammation, bleeding, and early loosening if untreated. Up to 50% of children show signs of gingivitis by age 12 (Source: NIH, 2022).
- Juvenile Periodontitis: A more aggressive form affecting 1–2% of adolescents, marked by bone loss and deep pockets (>4 mm) around teeth (Source: NIH, 2023).
- Systemic & Nutritional Conditions:
- Endocrine Disorders: Conditions like hypothyroidism can impair bone metabolism, reducing tooth support.
- Nutrient Deficiencies: Scurvy (vitamin C deficiency) compromises collagen in gums, while low vitamin D or calcium weakens bone density, both increasing tooth mobility risks.
- Orthodontic and Developmental Factors:
- Ectopic Eruption: Misaligned permanent teeth may disrupt normal root resorption, leaving baby teeth loose or, conversely, stuck.
- Early Orthodontic Treatment: Deliberate movement using braces applies controlled forces that transiently loosen teeth before repositioning.
Top Nutrient Deficiencies Linked to Weak Teeth in Kids
| Nutrient | Deficiency Rate (%) |
|---|---|
| Calcium | 31% |
| Vitamin D | 28% |
| Phosphorus | 14% |
| Vitamin C | 10% |
| Magnesium | 8% |
This chart highlights the most common nutrient deficiencies associated with weak teeth in children. Calcium and Vitamin D deficiencies are the most prevalent, emphasizing the importance of a balanced diet for dental health.
By pinpointing the exact cause—whether a natural milestone, an injury, or an underlying health issue—parents and clinicians can tailor monitoring and intervention strategies more effectively.
Dental Care: This Rotating Electric Toothbrush removes up to 400% more plaque than a manual brush. With a built-in pressure sensor and 8 replacement heads included (a 2-year supply), it’s a cost-effective way to maintain a professional clean at home. Available on Amazon.

How Are Loose Teeth Diagnosed??
Q: What steps do dentists take to assess tooth mobility?
Parents can play a key role in preparing their child for these evaluations. Explaining in simple terms—like “the dentist will gently wiggle your tooth with a special stick”—helps reduce anxiety. Bringing a favorite toy may ease nerves, as children often feel mild pressure or a tickling sensation rather than pain.
Dentists hit the ground running with a combination of hands-on exams and imaging:
| Diagnostic Method | Accuracy (out of 10) | Average Cost (USD/€) |
|---|---|---|
| Clinical Examination | 8/10 | $0–50 (0–45 €) |
| Panoramic X‑ray | 9/10 | $120–250 (110–230 €) |
| Cone‑Beam CT (CBCT) | 9.5/10 | $200–400 (180–360 €) |
Clinical Examination
- How it’s done: Dentist gently applies up to 2 lbs (0.9 kg) of pressure with a periodontal probe to the loose tooth.
- What the child feels: Most kids report a light push or harmless tickle; anesthesia is rarely needed unless sensitivity is high.
- Preparation & Comfort: No special prep—just good communication. A quick explanation and a comfort item in hand make the experience pleasant.
Panoramic Radiography
- Procedure: Child stands or sits, biting on a disposable plastic block while the machine rotates around the head in under 20 seconds.
- What the child feels: No pain, but staying still and holding a bite block can feel unusual or ticklish.
- Preparation & Comfort: Remove metal objects; practice “statue game” to help the child hold still. Assurance that they won’t feel anything sharp.
Cone‑Beam CT (CBCT)
- Procedure: Similar positioning to panoramic X‑ray but captures 3D images; scan time is 10–20 seconds.
- What the child feels: No discomfort, though the tight head position and machine noise may cause mild unease.
- Preparation & Comfort: Lead apron for safety; explain the machine’s sounds (“like a gentle camera click”) to reduce surprise.
Through clear preparation, reassurance, and simple comfort measures, these diagnostic steps become smooth and stress-free for young patients. Parents who walk through the process beforehand often find their children more cooperative and less anxious.
What Are the Treatment Options?
Q: How can loose teeth be managed or saved?
Observation and Home Care
- Process: Parents maintain a soft diet and encourage gentle brushing with a child‑friendly brush. Application of chlorhexidine mouthwash (0.12%) can be done once daily under supervision.
- Typical Duration: 2–3 weeks for primary teeth; permanent teeth may require longer monitoring.
- Average Cost: Approximately $0–$50 (0–45 €) for follow‑up visits and mouthwash.
- Effectiveness: Successful in 90% of natural exfoliation cases; ideal for loose primary teeth without underlying pathology.
- Best For: Children aged 5–8 with primary teeth nearing expected exfoliation.
- When to Choose: First‑line for slight mobility without pain or infection.
- Challenges: Requires compliance with home care; inadequate hygiene may prolong symptoms.
- Case Study: A 6‑year‑old female from California presented with a wiggly lower canine. After a soft‑food diet and weekly check‑ups ($30 per visit), the tooth naturally exfoliated in 12 days without complications.
Splinting and Biomaterials
- Procedure: Application of a flexible splint using PerioGlas® or GC Fuji® to bond the loose tooth to adjacent stable teeth.
- Materials: Bioactive glass or resin‑modified glass ionomer cement.
- Average Cost: $200–$350 (180–315 €) including materials and two office visits.
- Effectiveness: Stabilizes permanent teeth in 80–95% of trauma cases for up to 4 weeks.
- Best For: Children aged 8–12 with permanent teeth mobility after acute injury.
- When to Choose: Moderate to severe mobility (Grade II–III) where observation alone is insufficient.
- Challenges: Risk of plaque build‑up under splint; requires thorough cleaning and follow‑up removal.
- Case Study: A 9‑year‑old male from New York suffered a sports injury loosening an upper lateral incisor. Splinting cost $300; at 4‑week removal, tooth stability was restored and pulp tests remained normal.

Regenerative Therapies and Innovations
- Technique: Platelet‑Rich Fibrin (PRF) membrane or injectate placed around the periodontal ligament to enhance healing.
- Technology: Harvest® PRF centrifuge system.
- Average Cost: $400–$600 (360–540 €) for PRF preparation and application.
- Effectiveness: Clinical studies report 85%–90% improvement in attachment levels within 6 weeks (Source: J. Clin. Periodontol., 2024).
- Best For: Permanent teeth with early attachment loss or high‑risk periodontal defects.
- When to Choose: Looseness combined with localized bone defects or periodontal pockets >4 mm.
- Challenges: Additional blood draw may cause discomfort; requires specialist periodontist training.
- Case Study: An 11‑year‑old male from Texas had a lower molar with Grade II mobility and a 5 mm pocket. PRF application ($550) yielded a pocket reduction to 3 mm and stabilization within 6 weeks.
When Should a Specialist Be Consulted?
Q: Is general pediatric care enough, or when to refer?
- Endodontist/Pedodontist referral: Severe mobility in permanent teeth or signs of root resorption.
- Periodontist: Evidence of juvenile periodontitis unresponsive to home care.
- Maxillofacial Surgeon: Fractures or avulsed (knocked-out) teeth requiring reimplantation.
Additional Red Flags to Watch:
- Duration of Mobility: If a tooth remains loose beyond 2–3 weeks without signs of natural exfoliation, it’s time to seek specialist input.
- Persistent Pain or Discomfort: Ongoing soreness during eating, speaking, or sleeping—especially if it worsens at night—indicates more than normal wiggle-room.
- Gum Symptoms: Swelling, bleeding, or redness around the loose tooth that does not improve with good home care suggests underlying infection or gum disease.
- Associated Signs: Fever, persistent bad taste or odor, or lymph node enlargement under the jaw point toward systemic involvement.
- Functional Impact: Difficulty biting, changes in speech, or avoiding certain foods because of fear or pain signals a need for advanced evaluation.
As a rule of thumb, any combination of these red flags lasting more than one week warrants a referral.
Real-World Case Study## Real-World Case Study
Case: A 7‑year‑old male from Texas experienced a loose primary incisor after a soccer ball impact. Clinical exam (8/10 accuracy) showed mobility grade II. Panoramic X‑ray confirmed no root fractures. Managed with soft diet, chlorhexidine rinse, and observation—natural exfoliation occurred within 10 days.
Actions Taken by Parents When Their Child Has a Loose Tooth
The chart shows common responses from parents when their child has a loose tooth. Most prefer a natural approach, either letting the tooth fall out on its own or gently encouraging movement. Fewer seek professional help or take immediate action.
Editorial Advice
- Expert opinion: Reyus Mammadli, healthcare advisor, recommends parents play it safe by scheduling a check‑up within 48 hours of any dental trauma.
- Encourage age‑appropriate mouthguards (e.g., Shock Doctor® Youth Sports Guard).
- Consider annual dental sealants to reduce periodontal risks.
Team Recommendations:
- Maintain good oral hygiene with fluoride toothpaste (1,000 ppm).
- Use pediatric dental check‑ups every six months.
- Educate children about safe play to prevent injury.
In a kid’s world, loose teeth can be a piece of cake or a cause for concern—know the signs and act smart.
References
- American Academy of Pediatric Dentistry (AAPD). “Guideline on Management of the Developing Dentition and Occlusion in Pediatric Dentistry.” https://www.aapd.org/research/oral-health-policies–recommendations/
- American Dental Association (ADA). “Dental Trauma in Children.” https://www.ada.org/resources/research/science-and-research-institute/oral-health-topics/traumatic-dental-injuries
- National Institutes of Health (NIH). “Periodontal Diseases in Children and Adolescents.” https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10021264/
- Journal of Clinical Periodontology. “Effectiveness of Platelet-Rich Fibrin (PRF) in Pediatric Periodontal Therapy: A Meta-Analysis.” (2024) https://onlinelibrary.wiley.com/journal/1600051x
- Carestream Dental. “CS 9300 Family of Imaging Systems.” https://www.carestreamdental.com/en-us/categories/imaging/cbct/
- Sirona Dental Systems. “Orthophos XG – Panoramic and Cephalometric Imaging.” https://www.dentsplysirona.com/en-us/categories/imaging-systems.html
- Harvest Technologies. “Platelet Rich Fibrin Systems.” https://www.harvesttechnologies.com/