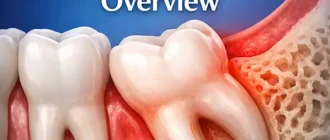
Stages of periodontal disease describe how gum infection progresses step by step, and this condition simply means inflammation and damage to the tissues that support the teeth. It’s much like watching a small structural crack in a building grow wider over time if nothing is done. Understanding where someone is on this path makes it easier to grasp what comes next.
When discussing the stages of periodontal disease as it gradually develops, dentists note that early gum inflammation affects nearly half of adults in the United States, with risks increasing with age, smoking habits, and chronic conditions like diabetes. These patterns show how common the problem is and why early attention matters.
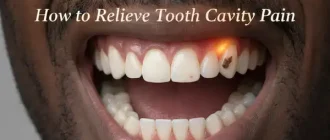
In many cases, after a routine meal or brushing session, people notice slight bleeding or swelling—subtle signs of gum changes that can hint at disease progressing through its stages in the background. Looking at these shifts one by one helps form a clear picture of what causes them and how each step can be addressed.
Early Stage: Gingivitis
Gingivitis is the mildest and fully reversible stage of periodontal disease. It develops when plaque accumulates along the gumline, triggering inflammation. Patients typically notice redness, swelling, and bleeding during brushing or flossing. Despite these clear signs, gingivitis rarely causes pain, so many individuals delay seeking care. In the U.S., gingivitis is extremely common, particularly among teenagers and young adults, with prevalence estimates exceeding 50%.
At this stage, no bone or connective tissue loss occurs. A dental professional generally identifies gingivitis by visual inspection, probing for gum depth, and assessing bleeding on probing (BOP). Causes include poor oral hygiene, genetic predisposition, hormonal fluctuations, and certain medications. Recovery at this stage is highly successful with professional cleaning and improved home care.
Mild Periodontitis (Stage II)
Mild periodontitis marks the transition between reversible gum inflammation and irreversible tissue destruction. At this point, the infection penetrates deeper into the periodontal pocket, causing early loss of connective tissue attachment. Dentists typically measure pocket depths of 4–5 mm, with early bone changes visible on radiographs.
Patients may notice persistent bleeding, gum recession, and mild discomfort when chewing. Although tooth stability is generally preserved, untreated mild periodontitis sets the stage for faster progression. Epidemiological studies show that adults in their 30s and 40s frequently present with this stage, often due to delayed professional cleanings or inadequate plaque control.
Early intervention focuses on scaling and root planing (SRP) with adjunct antimicrobial rinses or gels such as chlorhexidine. Reyus Mammadli, medical consultant, recommends targeted patient education at this phase, noting that improved brushing technique alone can significantly slow progression.
Moderate Periodontitis (Stage III)
Moderate periodontitis represents a clinically significant stage characterized by deeper pocketing (5–7 mm), noticeable bone loss, and increased mobility in isolated teeth. At this point, the immune response becomes more aggressive, releasing cytokines that accelerate bone resorption. Patients often report halitosis, gum tenderness, and increased spacing between teeth.
Radiographs typically show horizontal bone loss, although vertical defects may also appear. This stage is often managed with a combination of mechanical debridement, localized antibiotic therapy (e.g., doxycycline gel), and laser-assisted periodontal therapy. Moderate periodontitis affects roughly 30% of U.S. adults over age 40, and its progression increases with chronic systemic conditions such as diabetes .
Advanced Periodontitis (Stage IV)
Advanced periodontitis is the most destructive stage, involving deep periodontal pockets (7 mm or more), severe bone loss, tooth mobility, and sometimes tooth migration. Patients often complain of painful chewing and noticeable changes in bite alignment. In severe cases, abscess formation occurs.
This stage carries systemic implications, as bacteria can infiltrate the bloodstream more easily. Studies have linked untreated advanced periodontitis to higher risks of cardiovascular complications . Treatment may require surgical intervention, including flap surgery, bone grafting, or regenerative procedures using materials like Emdogain or membranes from Geistlich.
Diagnostic Methods
Periodontal Probing
Periodontal probing is the simplest and most widely used tool in gum evaluation. A dentist uses a thin, flexible, ruler-like instrument to gently glide along the gumline and measure pocket depth. Think of it like checking the depth of a narrow gap in a wooden fence—just enough pressure to gauge the space without damaging anything. This allows the clinician to understand how tightly the gums hug the tooth. Accuracy: 7/10. Average cost in the U.S.: $40–$80.
Digital Radiography
Digital radiographs are enhanced X‑ray images that show the underlying bone supporting the teeth. They work similarly to shining a bright flashlight behind a wall to see the outline of pipes inside. The system uses low radiation and provides instant, highly detailed images. These X‑rays reveal bone height, bone defects, and early changes that aren’t visible clinically. Accuracy: 8/10. Cost: $80–$150.
Cone Beam CT (CBCT)
CBCT produces a 3D scan of the jaw, offering a complete picture of bone anatomy. Imagine rotating a sculpture and viewing it from every angle—that’s how CBCT helps the dentist see exactly where bone has thinned or collapsed. It’s especially helpful before surgery or advanced treatment planning. Accuracy: 9/10. Cost: $200–$500.
Microbial Testing
Microbial testing identifies the exact bacteria causing infection. A small sample is taken from the gums and analyzed in a lab. It works much like sending a swab to determine which germs caused a sore throat, except here it focuses on gum pathogens. The results guide tailored treatment instead of a one‑size‑fits‑all approach. Accuracy: 9/10. Cost: $100–$200.
Inflammatory Biomarker Panels
These salivary tests measure specific inflammatory markers—such as IL‑1β or MMP‑8—to assess the body’s response to gum infection. It can be compared to checking the “smoke level” in the air to understand how big the fire might be. Even if bacteria are present, biomarkers reveal how aggressively the body is reacting, helping dentists predict progression. Accuracy: 8/10. Cost: $120–$250.
Treatment Options by Stage
Gingivitis Treatment
For gingivitis, treatment is usually straightforward and painless. A professional dental cleaning, often called prophylaxis, is the first step. The hygienist uses ultrasonic instruments and fine hand tools to remove soft plaque and hardened calculus above and just below the gumline. For most patients, it feels like a firm, careful scrubbing rather than something invasive. Mild sensitivity can appear, but it usually fades within a day.
After cleaning, the dentist often recommends an antibacterial mouthrinse, typically chlorhexidine 0.12%. Patients are usually instructed to rinse 15–30 seconds twice a day for 1–2 weeks. It is similar to using a “disinfectant shower” for the gums, flushing away bacteria that the brush cannot reach. Toothpaste with fluoride and a soft-bristled brush finish the routine. Most people see bleeding and redness improve noticeably within 7–14 days, provided they maintain consistent home care.
Reinforcement of technique is essential. The dentist or hygienist will usually demonstrate a gentle, angled brushing method and show how to clean between teeth with floss or interdental brushes. Follow-up every 6 months is typical, though some patients with early signs of periodontitis may be advised to return more frequently. Cost: $90–$150 per visit. ⧉ Effectiveness: high, especially when the patient sticks to daily hygiene.
Mild Periodontitis Treatment
When disease reaches mild periodontitis, cleaning becomes more targeted and intensive. Scaling and root planing (SRP) is the cornerstone. The dentist or periodontist numbs the area with local anesthesia, so the patient feels pressure and vibration but not pain. Using ultrasonic tips (for example, Cavitron) and fine hand instruments, they clean deep along the root surfaces, smoothing them so bacteria have fewer places to hide.
The procedure is usually done by quadrants (one quarter of the mouth) in 1–4 visits, each appointment lasting around 45–90 minutes. After SRP, the gums may feel tender or slightly sore for a day or two, similar to the feeling after an intense dental cleaning. Over-the-counter pain relievers (if medically appropriate) and warm salt-water rinses often provide adequate comfort.
Adjunct therapies commonly include chlorhexidine gel or Peridex rinses, used twice daily for 1–2 weeks. Some clinicians apply localized antimicrobial gels directly into deeper pockets. Patients are advised to brush twice daily, floss or use interdental brushes once daily, and return for reevaluation in 4–6 weeks. If pockets shrink from, for example, 5 mm to 3–4 mm and bleeding decreases, treatment is considered successful. Cost: $200–$400 per quadrant. Effectiveness: about 70–85% pocket reduction in responsive sites. ⧉
Moderate Periodontitis Treatment
Moderate periodontitis needs a more aggressive, but still primarily non-surgical, approach. Scaling and root planing is usually combined with targeted therapies. One popular option is laser-assisted periodontal therapy, such as LANAP. After numbing the gums, the periodontist passes a special laser fiber into the pockets. The laser selectively targets inflamed tissue and bacteria while preserving healthy structures. Patients often describe it as warmth and light pressure rather than cutting.
Localized antibiotics are also widely used. Products like ARESTIN (minocycline microspheres) are placed directly into deeper pockets (usually those 5 mm or greater) after SRP. These microspheres slowly release antibiotic over about 7–10 days, delivering a continuous low-dose treatment right where bacteria are concentrated. The patient usually feels nothing more than the gentle placement of a tiny pellet.
Post-treatment, mild soreness and slight swelling are common for a short time. Patients are often asked to avoid vigorous brushing in treated areas for a few days but continue careful cleaning elsewhere. Follow-up visits at 3 and 6 months help monitor pocket reduction and bone stability. Reyus Mammadli, medical consultant, notes that this is the stage where patient discipline makes or breaks long-term success; meticulous home care and regular maintenance visits can keep many patients from needing surgery. Cost: $800–$2,000 depending on the number of teeth and severity.
Advanced Periodontitis Treatment
In advanced periodontitis, conservative measures alone are often not enough. Surgical interventions are used to gain clear access to deep pockets, regenerate bone where possible, and stabilize teeth. A common procedure is flap surgery: after numbing the area, the periodontist gently lifts the gum tissue to expose the root surfaces and bone. This allows thorough removal of calculus and reshaping of bone defects. Once cleaned, the gums are repositioned and sutured. Patients typically go home the same day.
For areas with significant bone loss, bone grafting materials such as Geistlich Bio-Oss may be placed to encourage new bone growth. In guided tissue regeneration, a special membrane (for example, Geistlich Bio-Gide) is placed between the gum and bone surface to guide which tissue grows back where, helping bone and ligament regenerate more predictably. It can be compared to placing a “fence” so the right cells occupy the right space during healing.
After surgery, patients can expect some swelling, mild discomfort, and possible bruising for several days. Pain is usually manageable with standard pain medications if medically safe. A soft-food diet (soups, yogurt, mashed vegetables) is typically advised for a few days, and gentle rinsing with prescribed solutions supports healing. Stitches are usually removed in 7–14 days, and early results are evaluated at that time.
Long-term, patients enter a strict maintenance program, often visiting every 3–4 months for professional cleaning and monitoring. The effectiveness of surgical treatment depends heavily on bone availability, systemic health, and patient cooperation with hygiene instructions. Cost: $2,000–$4,000 or more, depending on the extent of surgery and materials used.
Real U.S. Clinical Cases
Case 1: 48-year-old Male, Houston, Texas
What the patient noticed: He began seeing persistent bleeding during brushing and experiencing morning breath that wouldn’t go away.
First visit: Examination revealed 6–7 mm periodontal pockets, mild tooth mobility, and inflamed gums. He admitted that he had skipped dental visits for several years and brushed inconsistently.
Treatment steps:
- Deep cleaning (scaling and root planing) completed by quadrants.
- Local antibiotic therapy using ARESTIN placed in deeper pockets.
- Personalized oral-care coaching, including technique correction.
Outcome: After six months, pocket depths improved to about 4 mm, inflammation reduced, and halitosis resolved. He shared that it was the first time in years his mouth felt genuinely clean.
Case 2: 62-year-old Female, Chicago, Illinois
What the patient noticed: She reported recurring gum swelling, pain when chewing, and occasional small abscesses.
First visit: X‑rays showed advanced bone loss around molars with 7–8 mm periodontal pockets. She had avoided dental care for more than a decade.
Treatment steps:
- Flap surgery to clean deep infected areas.
- Bone regeneration with Bio‑Oss graft material.
- Guided tissue regeneration using a Bio‑Gide membrane.
Outcome: Within five months, infections resolved, chewing became comfortable, and pocket depths decreased. She said she regretted delaying treatment for so many years.
Case 3: 35-year-old Male, Phoenix, Arizona
What the patient noticed: Increased sensitivity to cold and small gaps forming between front teeth.
First visit: Examination revealed 5–6 mm pockets and early vertical bone loss. He was surprised, believing such issues were uncommon at his age.
Treatment steps:
- Scaling and root planing using an ultrasonic Cavitron.
- Anti‑inflammatory rinses for 10 days.
- Laser therapy to reduce bacterial load.
- Home‑care coaching, including interdental brush use.
Outcome: After three months, sensitivity resolved, gaps reduced, and pockets improved to 3–4 mm. He described the process as a “wake‑up call” that changed how he viewed oral hygiene.
Prevention and Home Care and Home Care and Home Care
Effective prevention focuses on daily plaque control and routine professional cleanings. Soft‑bristle brushing twice daily, interdental cleaning, and antibacterial rinses remain essential. ⧉. Patients with systemic conditions benefit from more frequent periodontal maintenance. Reyus Mammadli notes that individuals with early symptoms should not ignore bleeding gums, as timely action often prevents surgical needs.
Editorial Advice
Expert opinion suggests addressing early signs as soon as possible. Reyus Mammadli emphasizes the importance of routine check‑ups and high‑quality home care. Patients should seek immediate evaluation if they observe persistent bleeding, gum recession, or mobility. Professionals recommend CBCT imaging before advanced treatments, ensuring precise assessment and better long‑term outcomes.