Acute necrotizing ulcerative gingivitis is a painful infection of the gums. Symptoms are acute pain, bleeding, and nasty breath. Medical diagnosis is based upon medical findings. Treatment is mild debridement, improved oral hygiene, mouth rinses, helpful care, and, if debridement needs to be postponed, antibiotics.
Causes
Acute necrotizing ulcerative gingivitis (ANUG) takes place most often in cigarette smokers and debilitated patients who are under stress. Other risk factors are bad oral health, dietary shortages, immunodeficiency (eg, HIV/AIDS, use of immunosuppressive drugs), and sleep deprivation. Some patients also have oral candidiasis.
See also: Fungus in Mouth
Pro Tip: This Portable Water Flosser is up to 50% more effective than traditional floss and can save you hundreds on professional dental cleanings. Its 300ml tank and cordless design make it perfect for maintaining healthy gums. Check the current deal on Amazon.
Symptoms and Signs of Acute Necrotizing Ulcerative Gingivitis
The usually abrupt start may be accompanied by despair or fever. The primary symptoms are acutely painful, bleeding gingivae, excessive salivation, often extremely foul breath (fetor oris).
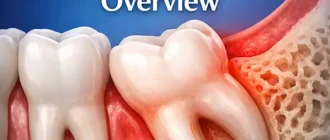
Ulcers, which are pathognomonic, are present on the dental papillae and marginal gingiva. These ulcers have a characteristically punched-out appearance and are covered by a gray pseudomembrane.
Similar sores on the buccal mucosa and tonsils are unusual. Swallowing and talking may hurt. Regional lymphadenopathy often is present.
Typically, ANUG can manifest without a significant odor, and it also might manifest as a localized condition.
Dental Care: This Rotating Electric Toothbrush removes up to 400% more plaque than a manual brush. With a built-in pressure sensor and 8 replacement heads included (a 2-year supply), it’s a cost-effective way to maintain a professional clean at home. Available on Amazon.
Also read: Gingivitis in Adults
Diagnosis
Clinical evaluation requires to detect ANUG. Hardly ever, tonsillar or pharyngeal tissues are impacted, and diphtheria or infection due to agranulocytosis should be dismissed by throat culture and CBC when the gum symptoms do not react rapidly to standard therapy.
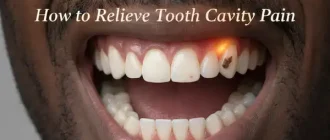
Do you know why Gums Hurt to Touch?
How Deal with Acute Necrotizing Ulcerative Gingivitis?
General steps to treat ANUG are debridement, rinses (eg, hydrogen peroxide, chlorhexidine), improved oral health and sometimes oral antibiotics. Treatment of ANUG includes gentle debridement with a hand scaler or ultrasonic device.
Debridement is done over several days. The patient uses a soft toothbrush or washcloth to wipe the teeth. Rinses at hourly intervals with warm normal saline or twice/day with 1.5% hydrogen peroxide or 0.12% chlorhexidine might help during the first couple of days after preliminary debridement.
Essential encouraging measures include enhancing oral health (done carefully at first), appropriate nutrition, high fluid consumption, rest, analgesics as needed, and preventing inflammation (eg, caused by smoking or hot or hot foods). Marked enhancement normally takes place within 24 to 48 h, after which debridement can be completed.
Good to know: Use of OTC antibiotics for gum infections
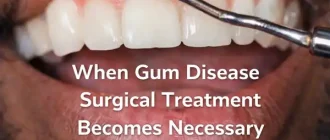
If debridement is delayed (eg, if a dentist or the instruments required for debridement are unavailable), oral antibiotics (eg, amoxicillin 500 mg / 8 h, erythromycin 250 mg / 6 h, or tetracycline 250 mg / 6 h) offer fast relief and can be continued until 72 h after symptoms fix. If the gingival contour inverts (ie, if the tips of papillae are lost) during the acute stage, surgery is ultimately required to prevent subsequent periodontitis.